In this analysis, I’m looking at some researches pertaining to the association between smoking and COVID-19
illness/mortality. There are number of studies ([1], [2], [3], [4]) that dig down
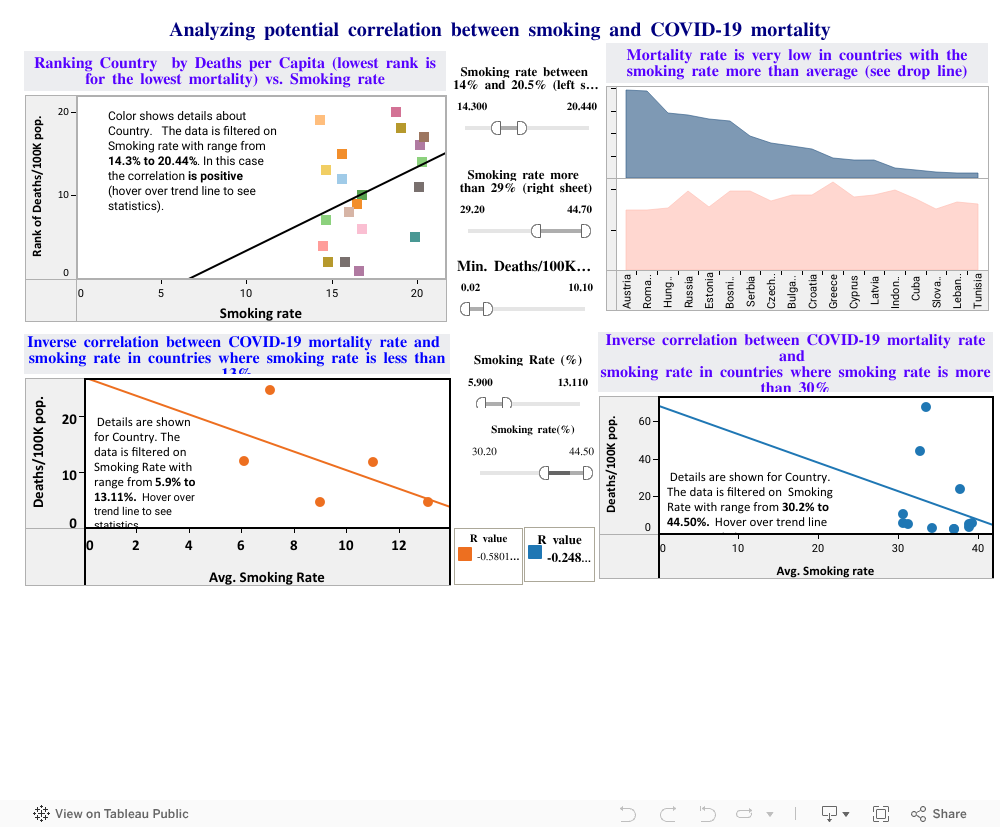
on smoking/COVID-19 mortality relationship and found some inverse trend between smoking and COVID-19 illness/mortality
(though, those studies are waiting for peer review).
Suggested mechanisms that may confer a protective effect of smoking include altered host cell expression of
angiotensin-converting enzyme 2 (ACE2, the receptor the virus uses to infects cells). Experimental data
pointed that infection with SARS-CoV and SARS-CoV-2 leads to down-regulation of ACE2 and this down-regulation
is detrimental due to uncontrolled ACE and angiotensin 2 activity. It has been observed that decreased ACE2
availability contributes to lung injury and ARDS development. More recent analyses suggest that up-regulation
of ACE-2 caused by smoking could be detrimental for COVID-19.
Therefore, higher ACE2 expression, while seemingly
paradoxical, may protect against acute lung injury caused by COVID-19. Other explanations include the
anti-inflammatory activity of nicotine; the antiviral effect of nitric oxide; the effects of smoking on the
immune system and vapor heat-related stimulation of immunity in the respiratory tract.
The study made by University of Washington and Stanford University School of Medicine [1] shown
that smokers are significantly under-represented among hospitalized COVID-19 patients in many countries where
smoking population prevailed. Another study [2] conducted by Sorbonne University medical team consisted of
gathering and analyzing statistics from patients hospitalized with COVD-19 in French clinics. They concluded that
active smokers may be protected against symptomatic COVID-19. This was evidenced for outpatients (who have less
serious infections) as well as for hospitalized patients.
The physio pathological process underlying this effect
may involve nicotine through the nicotinic receptor (and not the smoke of cigarettes per se). As it was mentioned
in article [4], “Since nicotine has been shown to activate the
Th2 branch of the immune response, it would be interesting to test if nicotine could mediate these effects through
the tilting of the Th1/Th2 immune branches towards Th2”.
But all studies stressed out that any of such hypothesis deserves further evidence and findings needs careful
consideration and cannot be translating into a clinical practice as it. Careful investigation of the potential
protective effect of nicotine should be investigated both in in vitro and in vivo before any firm conclusion can
be drawn. The interaction of smoking and COVID-19 will only be reliably determined by carefully designed
prospective study, and there is reason to believe that there are unknown confounds that may be spuriously
suggesting a protective effect of smoking.